When healthcare providers respond to a cardiac arrest, the basic tools of resuscitation often look the same: chest compressions, ventilations, airway management, and advanced life support interventions. However, one of the most important lessons taught in Pediatric Advanced Life Support (PALS) is that children are not simply small adults.
The reason is rooted in physiology. Most adult cardiac arrests begin with a cardiac problem, while most pediatric cardiac arrests begin with a respiratory problem. This distinction changes how providers assess patients, prioritize interventions, manage airways, and deliver ventilations during resuscitation.
Understanding these respiratory differences is essential for healthcare professionals, students, and emergency responders. Whether you are preparing for a PALS certification course or seeking to improve your clinical knowledge, understanding why pediatric patients deteriorate differently can help you recognize emergencies sooner and provide more effective care.
PALS vs Adult CPR: Quick Summary
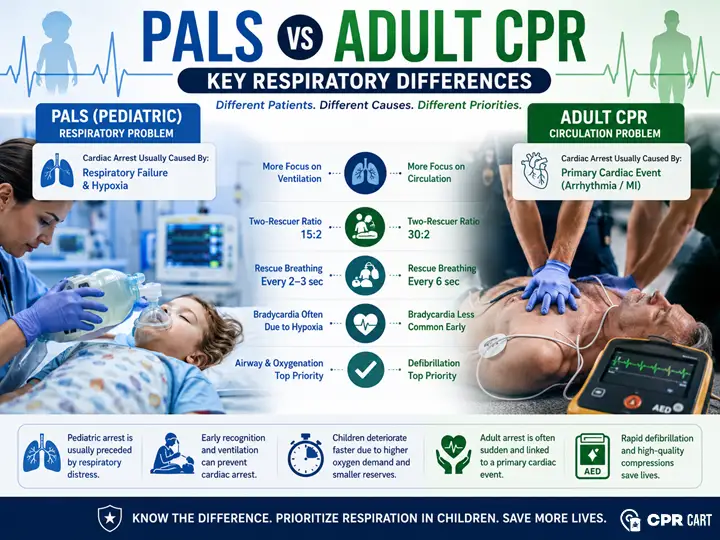
Pediatric cardiac arrest is usually caused by respiratory failure and hypoxia, whereas adult cardiac arrest is more commonly caused by a primary cardiac event. Because of this difference, PALS places greater emphasis on airway management, oxygenation, rescue breathing, and ventilation. Adult CPR focuses more heavily on maintaining circulation and early defibrillation.
Key differences include:
- Ventilation plays a larger role in pediatric resuscitation.
- Airway assessment becomes a priority earlier in PALS.
- Rescue breathing is emphasized more heavily in children and infants.
- Pediatric patients receive more frequent ventilations during two-rescuer CPR.
- Early recognition of respiratory failure can often prevent cardiac arrest.
Why Children Arrest Differently Than Adults
Adult cardiac arrest often occurs suddenly. A patient may experience a myocardial infarction, ventricular fibrillation, or another life-threatening arrhythmia and collapse with little warning. In these situations, restoring circulation and defibrillating shockable rhythms become immediate priorities.
Children typically follow a different path.
A child with severe asthma, bronchiolitis, pneumonia, airway obstruction, drowning, or sepsis usually deteriorates over time. When respiratory compromise occurs alongside circulatory dysfunction, providers must also recognize the early signs of shock. Learn more in our guide to PALS Shock Recognition and Management.
The body initially compensates by increasing respiratory effort and heart rate. As oxygen delivery becomes inadequate, respiratory failure develops. If intervention does not occur, hypoxia progresses to bradycardia, poor perfusion, and eventually cardiac arrest.
This progression explains why PALS training places such a strong emphasis on recognizing respiratory distress and respiratory failure before cardiac arrest occurs. In many pediatric emergencies, early airway support and effective ventilation can prevent the arrest altogether.
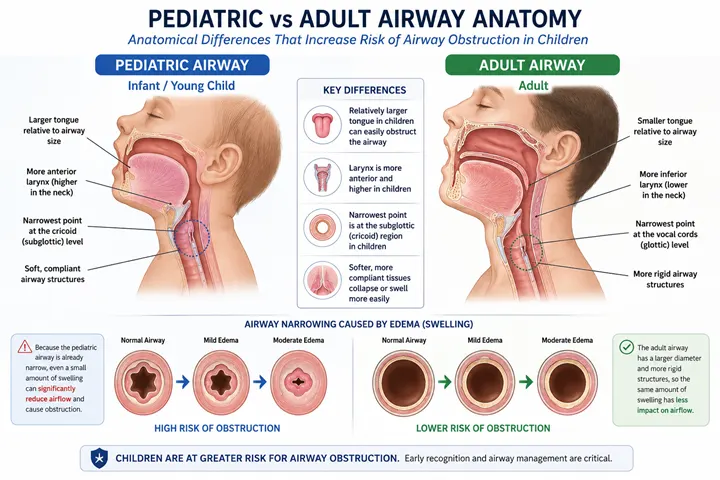
The Pediatric Airway: Small Changes Create Big Problems
Children have unique airway anatomy that makes respiratory emergencies more dangerous than many providers realize.
Compared with adults, children have:
- Smaller airway diameters
- Proportionally larger tongues
- A more anterior and cephalad larynx
- Less respiratory reserve
- Greater susceptibility to airway obstruction
While these differences may seem minor, they can dramatically affect airflow.
Clinical Pearl: Why Small Airway Swelling Is Dangerous
Children have much narrower airways than adults.
Even a small amount of swelling from croup, an allergic reaction, airway trauma, or infection can dramatically increase airway resistance and reduce airflow. This is why pediatric patients can develop respiratory distress and respiratory failure much faster than adults.
This principle helps explain why conditions such as croup, epiglottitis, anaphylaxis, and bronchiolitis can rapidly become life-threatening in young children.
Higher Oxygen Demand Means Less Time to Intervene
Children consume oxygen at a higher rate than adults relative to their body size. At the same time, they have smaller oxygen reserves within their lungs.
This combination means a child can become hypoxic much faster when breathing becomes ineffective.
Consider an infant with bronchiolitis who is struggling to breathe. While an adult may tolerate worsening respiratory distress for a longer period, a child can rapidly exhaust their respiratory reserve. Once respiratory muscles begin to fatigue, deterioration may occur within minutes.
This is why PALS providers are trained to recognize respiratory compromise before complete respiratory failure develops.
Signs of Impending Respiratory Failure
Providers should be alert for:
- Increased work of breathing
- Nasal flaring
- Retractions
- Grunting
- Poor air movement
- Cyanosis
- Altered mental status
- Decreasing responsiveness
When these findings appear, immediate intervention may prevent progression to cardiac arrest.
How the Cause of Arrest Changes CPR Priorities
The different causes of arrest in adults and children directly influence resuscitation priorities.
| Pediatric Cardiac Arrest | Adult Cardiac Arrest |
| Usually caused by respiratory failure and hypoxia | Usually caused by a primary cardiac event |
| Often preceded by respiratory distress | Frequently occurs suddenly |
| Bradycardia commonly develops before arrest | Ventricular arrhythmias commonly develop before arrest |
| Airway and ventilation are critical early interventions | Defibrillation and circulation are often immediate priorities |
| Prevention is often possible through early respiratory support | Prevention opportunities are frequently limited |
Understanding this distinction helps explain many of the protocol differences between PALS and adult CPR.
Compression-to-Ventilation Ratios: Why PALS Uses More Breaths
The respiratory focus of pediatric resuscitation is reflected in CPR compression-to-ventilation ratios.
For a single rescuer, both adult and pediatric CPR use:
30 compressions : 2 breaths
However, during two-rescuer CPR, the ratio changes for pediatric patients:
15 compressions : 2 breaths
Adults continue to receive:
30 compressions : 2 breaths
The increased ventilation frequency reflects the important role of hypoxia in pediatric cardiac arrest.
| Scenario | Adult CPR | Pediatric CPR |
| Single rescuer | 30:2 | 30:2 |
| Two rescuers | 30:2 | 15:2 |
| Advanced airway present | Continuous compressions | Continuous compressions |
| Ventilation rate with advanced airway | 1 breath every 6 seconds | 1 breath every 2–3 seconds |
Understanding how ventilation frequency changes with patient age is also important when comparing pediatric and adult airway management strategies. See Advanced Airways in BLS: How the CPR Ratio Changes for additional guidance.
Rescue Breathing Plays a Larger Role in PALS
One of the clearest examples of the respiratory focus of PALS is the emphasis on rescue breathing.
A child who is unresponsive but still has a pulse may not be experiencing a circulatory emergency. The primary problem may be inadequate oxygenation and ventilation. Effective rescue breathing can often reverse the underlying issue before cardiac arrest occurs.
For adults with a pulse but inadequate breathing:
1 breath every 6 seconds
For infants and children with a pulse but inadequate breathing:
1 breath every 2–3 seconds
The higher ventilation rate reflects both increased oxygen demands and the respiratory origins of many pediatric emergencies.
Airway Management Becomes a Priority Earlier
In adult cardiac arrest, providers generally focus first on high-quality chest compressions and rapid defibrillation when indicated. Airway interventions remain important but are often secondary to restoring circulation.
In pediatric emergencies, airway assessment frequently becomes a priority much earlier because respiratory compromise is often the root cause of deterioration.
PALS providers are trained to rapidly identify:
- Upper airway obstruction
- Lower airway disease
- Respiratory failure
- Inadequate oxygenation
- Ineffective breathing
Correcting these problems early can prevent progression to cardiac arrest.
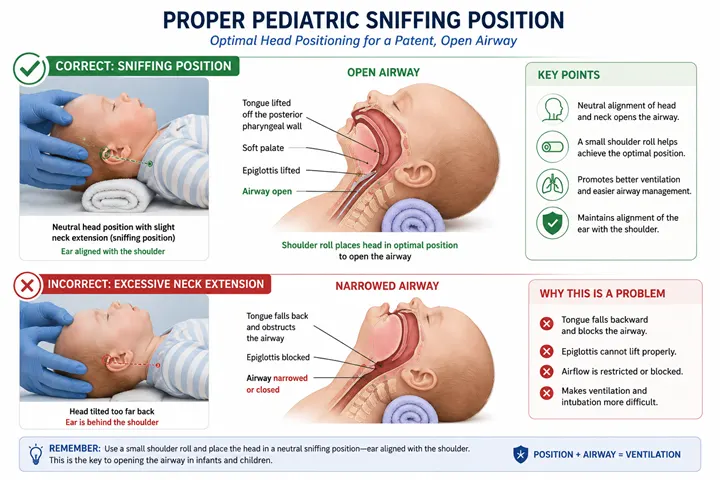
Clinical Pearl: The Sniffing Position Matters
Proper positioning can significantly improve ventilation.
Because of the unique anatomy of infants and children, placing the head in a neutral or slightly extended “sniffing” position often improves airway patency. Excessive neck extension may worsen airway obstruction, particularly in infants.
Why Hyperventilation Is Dangerous in Both Adults and Children
During resuscitation, providers often focus on ensuring adequate ventilation. However, excessive ventilation can significantly reduce CPR effectiveness.
Quantitative waveform capnography can help providers assess ventilation effectiveness and monitor CPR quality during advanced resuscitation. Learn more in Waveform Capnography in ACLS.
Clinical Pearl: Why Hyperventilation Is Harmful
More breaths are not always better.
Excessive ventilation increases pressure inside the chest, reducing venous blood return to the heart. During CPR, this can decrease cardiac output, lower coronary perfusion pressure, and reduce the effectiveness of resuscitation efforts.
This is why current resuscitation guidelines emphasize controlled ventilation rates and caution against aggressive bag-mask ventilation.
The goal is effective oxygenation, not excessive ventilation.
What Experienced PALS Providers Watch For
One of the biggest differences between novice and experienced providers is the ability to recognize deterioration before cardiac arrest occurs.
Experienced PALS providers often focus on subtle warning signs such as increasing work of breathing, worsening fatigue, poor air movement, altered mental status, and progressive bradycardia.
These findings frequently indicate that respiratory compensation is failing.
In many pediatric emergencies, the most important intervention is not what happens during cardiac arrest. It is recognizing respiratory failure early enough to prevent the arrest from occurring at all.
Conclusion
The key respiratory difference between PALS and adult CPR is rooted in the cause of cardiac arrest itself. Adult arrests are often sudden cardiac events that require immediate circulatory support and defibrillation. Pediatric arrests are frequently the final stage of progressive respiratory failure and hypoxia.
Consequently, PALS places greater emphasis on airway management, oxygenation, ventilation, and early recognition of respiratory compromise. Healthcare providers who understand these distinctions are better equipped to intervene early, prevent deterioration, and improve outcomes for critically ill children.
Frequently Asked Questions
What is the biggest respiratory difference between PALS and adult CPR?
The biggest difference is that pediatric cardiac arrest is usually caused by respiratory failure and hypoxia, while adult cardiac arrest is more commonly caused by a primary cardiac event. As a result, ventilation and airway management receive greater emphasis in PALS.
Why does pediatric CPR use a 15:2 ratio with two rescuers?
The 15:2 compression-to-ventilation ratio allows more frequent ventilations because respiratory failure and hypoxia commonly contribute to pediatric cardiac arrest.
Are rescue breathing rates different in PALS and adult CPR?
Yes. Adults with a pulse but inadequate breathing receive one breath every 6 seconds, while infants and children receive one breath every 2 to 3 seconds.
Why is bradycardia so important in pediatric emergencies?
Bradycardia in children is often caused by worsening hypoxia. Correcting oxygenation and ventilation can improve heart rate and help prevent progression to cardiac arrest.
Why can children deteriorate faster during respiratory emergencies?
Children have higher oxygen demands, smaller oxygen reserves, and narrower airways. These factors allow hypoxia to develop more rapidly than in adults.
Is ventilation more important than chest compressions in pediatric CPR?
Both are essential. However, because respiratory failure commonly contributes to pediatric cardiac arrest, ventilation plays a larger role in pediatric resuscitation than it does in many adult cardiac arrests.