In pediatric emergencies, a child’s condition can deteriorate with frightening speed. For healthcare providers, recognizing the shift from compensated to decompensated shock is the difference between a successful resuscitation and cardiopulmonary arrest.
According to Pediatric Advanced Life Support (PALS) guidelines, shock is inadequate tissue perfusion and oxygen delivery to meet metabolic demands. Children have robust compensatory mechanisms, meaning they can mask severe illness until they hit a physiological cliff.
Understanding shock recognition is a critical skill taught during a PALS certification course. This guide breaks down how to identify the early signs of decompensated shock, preventing the progression to irreversible organ damage.
What is Decompensated Shock in PALS?
Decompensated shock occurs when a child’s homeostatic mechanisms (like intense tachycardia and systemic vasoconstriction) can no longer maintain adequate perfusion to vital organs, specifically failing to sustain a normal blood pressure.
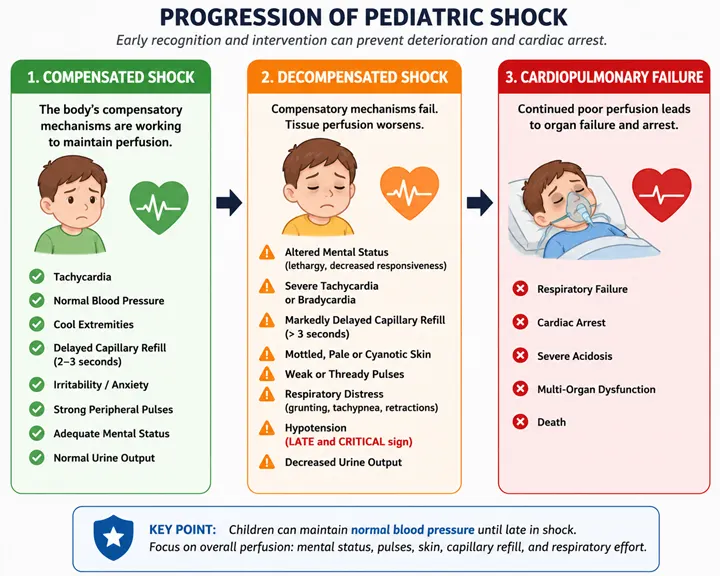
In the initial stages known as compensated shock, a child may look highly irritable, pale, or have a fast heart rate, but their body is successfully keeping their blood pressure within a normal range. Once those defenses fail, the child enters decompensated shock.
Decompensated shock in pediatrics is an advanced stage of shock where the body’s compensatory mechanisms fail to maintain adequate tissue perfusion, leading to hypotension (low blood pressure), altered mental status, and severe organ dysfunction. Unlike adults, children maintain a normal blood pressure for a long time during shock; therefore, hypotension is a late, critical sign of impending cardiac arrest.
The Core Difference: Compensated vs. Decompensated
The clinical dividing line between these two states is systolic blood pressure.
- Compensated Shock: Signs of poor perfusion (delayed capillary refill, cool extremities) are present, but blood pressure is normal.
- Decompensated Shock: Signs of poor perfusion are accompanied by hypotension.
For more details, read our guide on Pediatric Shock in PALS: Compensated vs. Decompensated
Why Early Recognition of Decompensated Shock Matters
Children often deteriorate rapidly once compensatory mechanisms fail. When decompensated shock is not recognized early, inadequate tissue perfusion can lead to metabolic acidosis, organ dysfunction, respiratory failure, and ultimately cardiac arrest. Prompt identification allows healthcare providers to intervene before irreversible injury occurs.
Early Signs of Decompensated Shock
While hypotension is the formal diagnostic marker, waiting for a blood pressure drop to occur means you are already behind. Excellent clinical performance requires catching the transition just as compensation fails. Watch for these progressive clinical indicators:
1. Altered Mental Status (Critical Early Indicator)
As brain perfusion drops, a child’s neurological status shifts. A previously irritable, crying child who becomes surprisingly quiet, lethargic, or difficult to arouse is demonstrating a severe lack of cerebral oxygenation. Look for:
- Decreased responsiveness to parents or painful stimuli.
- A vacant stare or inability to focus.
- Flaccid muscle tone.
2. The Shift in Heart Rate (Tachycardia to Bradycardia)
While marked tachycardia (an abnormally fast heart rate) is a hallmark of early compensation, an exhausted myocardium (heart muscle) will eventually slow down.
- The Warning Sign: Persistent tachycardia that transitions toward relative bradycardia in a child who remains poorly perfused should raise concern for impending cardiovascular failure.
- The Danger Sign: Bradycardia (a slow heart rate) in a symptomatic, poorly perfused child is an ominous, late sign of decompensation and a precursor to cardiac arrest.
3. Profound Skin Changes and Central Cyanosis
In compensated shock, the body shunts blood away from the skin to protect the brain and heart, causing cool, pale extremities. In decompensated shock, this mechanism fails completely:
- Skin becomes cold, clammy, and deeply mottled throughout the trunk, not just the limbs.
- Central cyanosis (bluish tint to the lips, tongue, and core) develops as hemoglobin deoxygenates heavily before even leaving the central circulation.
- Capillary refill time is significantly prolonged (greater than 3 seconds) or completely absent.
4. Respiratory Failure (Gasping or Grunting)
Respiratory effort increases drastically as the body tries to compensate for metabolic acidosis (built-up lactic acid from oxygen-starved tissues). As the child decompensates, you will observe:
- Extremely rapid, shallow breathing (tachypnea) transitioning to irregular or slow breathing.
- Grunting: An expiratory sound made as the child tries to keep their alveoli open to maximize oxygen exchange.
- Head bobbing or severe intercostal retractions.
Defining Hypotension by Age (PALS Criteria)
To accurately identify decompensated shock, you must know what constitutes a low systolic blood pressure across different pediatric age brackets. Memorizing the PALS formula for children aged 1–10 years is essential for rapid bedside calculations.
| Age Group | Systolic Blood Pressure (Hypotension Threshold) |
| Neonates (0–28 days) | less than 60 mmHg |
| Infants (1–12 months) | less than 70 mmHg |
| Children (1–10 years) | less than 70 mmHg + (2 × age in years) |
| Children (greater than 10 years) | less than 90 mmHg |
Immediate PALS Interventions for Decompensated Shock
When a child presents with decompensated shock, execution of the PALS algorithms must be flawless and immediate.
1. High-Flow Oxygen and Airway Support:
Immediate oxygen delivery and airway management are priorities in children with decompensated shock. Administer 100% high-flow oxygen via a non-rebreather mask. Prepare to support ventilation with a bag-mask device if the child shows signs of respiratory fatigue or altered mental status.
2.Establish Vascular Access: Within 5 Minutes.
Attempt rapid intravenous (IV) access. If dependable IV access cannot be established within 90 seconds or 3 attempts in an unstable child, immediately place an Intraosseous (IO) needle into the bone marrow.
3.Aggressive Fluid Resuscitation: First 15-30 Minutes.
Administer an immediate fluid bolus of 20 mL/kg of an isotonic crystalloid (e.g., Normal Saline or Lactated Ringer’s) over 5 to 10 minutes. Push the fluid rapidly via a syringe-stopcock setup rather than letting it gravity drip. Note: Reduce fluid volume to 5–10 mL/kg if cardiogenic shock is suspected.
4.Reassess and Repeat: Ongoing.
Evaluate the patient after every bolus. Check blood pressure, mental status, and heart rate. Prepare to administer up to 3 boluses (totaling 60 mL/kg) if no signs of fluid overload (e.g., hepatomegaly, rales) appear.
5.Initiate Vasoactive Medications: If Fluid-Refractory.
If hypotension persists despite adequate fluid resuscitation, initiate vasoactive support. Utilize epinephrine or norepinephrine infusions titrated to blood pressure and perfusion targets depending on whether it is “cold” or “warm” shock.
Why Hypotension Is a Late Sign of Pediatric Shock
Unlike adults, children can maintain blood pressure for an extended period through intense vasoconstriction and tachycardia. Although these compensatory mechanisms temporarily preserve circulation, tissue perfusion may already be significantly impaired. As a result, hypotension often appears late in pediatric shock and may indicate impending cardiovascular collapse.
Key Takeaways
Decompensated shock represents a critical stage of circulatory failure in which the body’s compensatory mechanisms can no longer maintain adequate tissue perfusion.
Early identification of decompensated shock can make a life-saving difference in pediatric emergencies. If you want to build confidence in pediatric assessment, shock recognition, and resuscitation principles, visit our PALS Certification page to learn more about available training options.
Frequently Asked Questions
What is the earliest sign of decompensated shock in a child?
Changes in mental status and worsening perfusion indicators are often among the earliest warning signs. Tachycardia, delayed capillary refill, and cool extremities frequently appear before hypotension develops.
Is hypotension always present in pediatric shock?
No. Children can maintain normal blood pressure for a prolonged period through compensatory mechanisms. Hypotension is generally considered a late sign of severe shock.
Why is pediatric shock harder to recognize than adult shock?
Children compensate effectively through increased heart rate and vasoconstriction. As a result, blood pressure may remain normal despite significant circulatory compromise.
What are the most common causes of shock in children?
Hypovolemia from dehydration is the most common cause. Other important causes include sepsis, cardiogenic conditions, and obstructive processes.
How quickly can compensated shock become decompensated?
The progression can occur rapidly, especially in infants and young children. Continuous reassessment is essential because deterioration may occur within minutes to hours.
Why does PALS emphasize perfusion assessment?
Perfusion indicators often reveal shock before hypotension develops. Assessing mental status, pulse quality, skin signs, capillary refill, and respiratory effort allows earlier recognition and intervention.