Pediatric Advanced Life Support (PALS) requires healthcare providers to rapidly assess and treat critically ill children. Among the most essential skills in the PALS toolbox is the management of tachycardia.
Unlike adult algorithms, pediatric tachycardia requires a nuanced approach because a rapid heart rate is often the body’s response to a stressor (like fear or fever) rather than a primary cardiac arrhythmia. This guide provides a deep dive into the PALS Tachycardia Algorithm, breaking down the decision-making process for identifying rhythm types and determining the appropriate intervention.
What is Pediatric Tachycardia?
Tachycardia in children is defined as a heart rate exceeding the normal range for the child’s age and activity level. However, the clinical significance depends heavily on the underlying cause. In PALS, we categorize tachycardia into two main types:
- Sinus Tachycardia: A physiologic response to pain, fever, hypovolemia, or anxiety. The treatment here is not anti-arrhythmic drugs; it is addressing the underlying cause.
- Arrhythmic Tachycardia: An abnormal electrical rhythm, such as Supraventricular Tachycardia (SVT) or Ventricular Tachycardia (VT).
Age-Specific Heart Rate Thresholds
To utilize the algorithm effectively, you must first determine if the heart rate is abnormally high for the patient’s age.
| Age Group | Normal Heart Rate (Awake) | Tachycardia Threshold |
| Newborn (0–1 mo) | 100–180 bpm | > 180 bpm |
| Infant (1–12 mo) | 100–180 bpm | > 180 bpm |
| Toddler (1–3 yrs) | 80–150 bpm | > 150 bpm |
| Preschool (3–6 yrs) | 70–120 bpm | > 140 bpm |
| School Age (6–12 yrs) | 60–100 bpm | > 120 bpm |
| Adolescent (>12 yrs) | 60–90 bpm | > 100 bpm |
The First Step: Clinical Assessment (Stable vs. Unstable)
Before memorizing drug dosages, the PALS Tachycardia Algorithm begins with a critical assessment of the patient’s hemodynamic stability. You must determine if the tachycardia is causing the patient to deteriorate.
Signs of Instability (Cardiopulmonary Compromise):
- Hypotension (Low blood pressure)
- Acutely altered mental status (lethargy, unresponsiveness)
- Signs of shock (pale, mottled skin, weak pulses)
- Acute heart failure (pulmonary edema, rales)
- Ischemic chest discomfort (rare in children, but possible)
If the patient is Unstable: The priority is immediate termination of the rhythm. Follow the Unstable Tachycardia with a Pulse pathway:
- Prepare for immediate synchronized cardioversion.
- Consider sedation if time permits, but do not delay shock.
- Start with 0.5 to 1 J/kg.
- If unsuccessful, increase to 2 J/kg.
If the patient is Stable: You have time to analyze the ECG rhythm. You must determine the QRS width to navigate the algorithm correctly.
“Learn how to rapidly identify these signs of distress using the Pediatric Assessment Triangle (PAT).
Analyzing the Rhythm: Narrow vs. Wide QRS
Once stability is established, look at the QRS complex on the ECG. This distinction dictates the treatment pathway.
1. Narrow-Complex Tachycardia (QRS < 0.09 seconds)
A narrow QRS indicates the impulse is originating above the ventricles (Supraventricular).
Differentiating Sinus Tachycardia from SVT:
This is the most critical decision point in the algorithm.
- Sinus Tachycardia: The rate varies with stimuli (e.g., slows down with comfort). History often reveals a cause like fever or dehydration. P waves are present and normal.
- SVT: The rate is often fixed (e.g., constantly 220 bpm) and does not respond to calming or pain control. P waves are often absent or hidden.
Management of Stable Narrow-Complex Tachycardia:
- If Sinus Tachycardia: Treat the underlying cause (oxygen, fluids, antipyretics).
- If SVT: * Vagal Maneuvers: First-line intervention. Use ice to the face (diving reflex) in infants.
- Adenosine: If vagal maneuvers fail. Initial Dose: 0.1 mg/kg (Max 6 mg). Second Dose: 0.2 mg/kg (Max 12 mg).
2. Wide-Complex Tachycardia (QRS > 0.09 seconds)
A wide QRS suggests the impulse originates from the ventricles or conducts abnormally.
Management of Stable Wide-Complex Tachycardia:
Expert consultation is highly recommended. The treatment often depends on whether the rhythm is monomorphic or polymorphic.
- Amiodarone: 5 mg/kg IV/IO over 20–60 minutes.
- Procainamide: 15 mg/kg IV/IO over 30–60 minutes.
- Caution: Do not use Procainamide and Amiodarone simultaneously as it can lead to severe hypotension.
“In wide-complex emergencies, establishing access is critical. Read more on IO vs. IV Access in Pediatric Emergencies.”
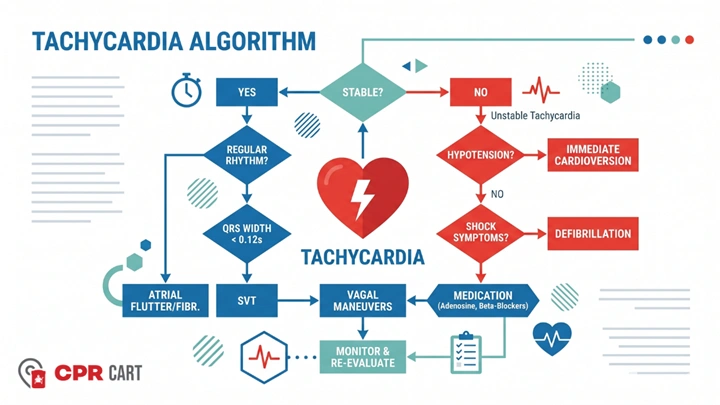
The PALS Tachycardia Algorithm Flowchart Summary
For quick reference, here is the logic flow of the algorithm:
- Identify Tachycardia: HR > normal for age.
- Assess Stability: Is the patient hypotensive, altered, or in shock?
- YES (Unstable): → Synchronized Cardioversion (0.5–1 J/kg, then 2 J/kg).
- NO (Stable): → Analyze QRS Width.
- Narrow QRS (< 0.09 sec):
- Likely Sinus Tachycardia → Identify/treat cause.
- Likely SVT → Vagal Maneuvers → Adenosine.
- Wide QRS (> 0.09 sec):
- Likely VT → Consider Amiodarone or Procainamide (Consult Expert).
Special Considerations: Pediatric Adenosine Administration
Adenosine has an incredibly short half-life (less than 10 seconds), so technique is vital:
- Proximity: Administer the drug as close to the heart as possible (upper arm or central line).
- The “Two-Syringe” Method: Follow with a rapid, bolus saline flush ($5–10\ mL$) immediately after the drug.
- Be Prepared: Warn the team of a transient period of asystole (heart stopping) on the monitor—this is normal.
Conclusion
The PALS Tachycardia Algorithm is designed to guide providers through a high-stress scenario with a logical, step-by-step approach. By prioritizing the assessment of stability, you can significantly improve outcomes for pediatric patients.
Remember, the most common cause of tachycardia in children is sinus tachycardia resulting from an underlying respiratory or metabolic issue. Always look for the “why” before treating the rhythm.
Looking to practice these algorithms in a hands-on environment? Check out our PALS Certification Classes Near You to master your skills.