Prone CPR is cardiopulmonary resuscitation (CPR) performed while a patient remains lying face down (in the prone position). It is used when cardiac arrest occurs and immediately turning the patient onto their back would cause a dangerous delay in chest compressions or create significant clinical risk. Although standard CPR is performed with the patient supine, current resuscitation guidance supports prone CPR when rapid repositioning is not feasible.
Why Would a Patient Need CPR While Prone?
Most cardiac arrests occur with the patient in a supine position, allowing rescuers to perform conventional chest compressions over the sternum. However, modern healthcare settings increasingly encounter patients who are intentionally positioned prone for therapeutic or procedural reasons.
Prone positioning is commonly used during spinal surgery, neurosurgical procedures, and certain orthopedic operations. It is also frequently utilized in intensive care units for patients with severe respiratory failure, including acute respiratory distress syndrome (ARDS), because prone positioning can improve oxygenation and ventilation-perfusion matching.
If cardiac arrest occurs in these situations, stopping to reposition the patient may require multiple personnel, interrupt critical procedures, risk dislodging advanced airways, and significantly delay the initiation of CPR. Because survival decreases with every minute without effective circulation, immediate prone CPR may be the most appropriate intervention while preparations are made for further resuscitation.
Prone CPR may be considered in:
- Patients undergoing spinal surgery
- Neurosurgical procedures performed in the prone position
- Mechanically ventilated ICU patients receiving prone positioning therapy
- Morbidly obese patients who cannot be rapidly repositioned
- Patients with unstable spinal injuries
- Situations where turning the patient could dislodge critical equipment or compromise patient safety
How Do You Perform CPR on a Prone Patient?
Step 1: Recognize Cardiac Arrest
As with conventional BLS, begin by assessing responsiveness and breathing. If the patient is unresponsive and not breathing normally, activate the emergency response system and obtain an AED if available.
Healthcare professionals should assess for a pulse according to current BLS guidelines. If no pulse is detected within 10 seconds, chest compressions should begin immediately.
For a review of cardiac arrest recognition, see Adult BLS Algorithm.
Step 2: Determine Whether Immediate Repositioning Is Possible
Before beginning compressions, quickly evaluate whether the patient can be safely turned supine without delaying CPR.
If repositioning requires significant time, multiple providers, interruption of surgery, or poses a risk of airway loss, spinal instability, or device dislodgement, compressions should begin in the prone position without delay.
The priority is minimizing interruptions in circulation.
Step 3: Identify the Correct Compression Landmark
Proper hand placement is critical for effective prone CPR.
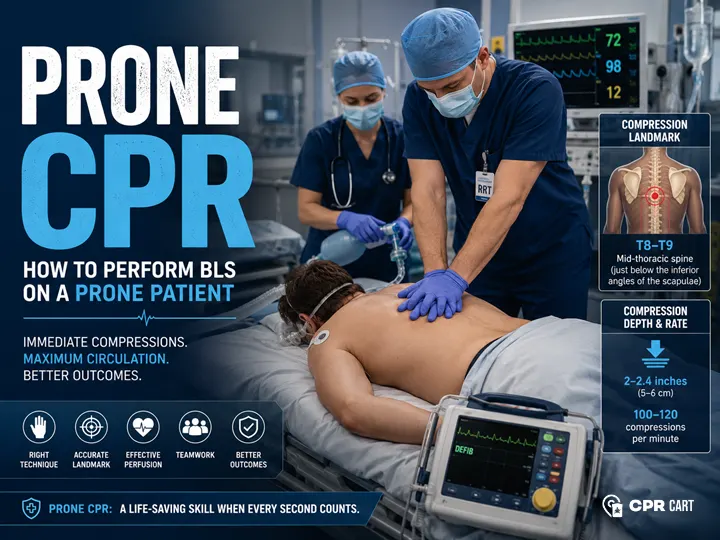
Current evidence suggests the optimal compression point is over the mid-thoracic spine, typically at the T8–T9 vertebral level. This landmark generally corresponds to a location just below the inferior angles of the scapulae in most adults.
Imaging studies evaluating cardiac anatomy in prone patients have demonstrated that this region most closely overlies the largest cross-sectional area of the left ventricle, allowing compressions to generate effective forward blood flow.
Place the heel of one hand directly over the T8–T9 region and position the second hand on top, using the same body mechanics employed during conventional CPR.
For additional guidance on compression landmarks, see adult CPR guidelines.
Step 4: Deliver High-Quality Chest Compressions
Once the compression landmark has been identified, begin compressions immediately.
Compression depth should remain consistent with current adult BLS recommendations: at least 2 inches but no more than 2.4 inches, delivered at a rate of 100–120 compressions per minute. Complete chest recoil should occur after each compression, and interruptions should be minimized whenever possible.
Although the direction of force differs from conventional CPR, the goal remains the same: generate adequate coronary and cerebral perfusion through effective cardiac compression.
Step 5: Provide Anterior Counter-Pressure When Possible
One of the most overlooked aspects of prone CPR is the importance of anterior counter-pressure.
Patients in operating rooms and intensive care units are often positioned on padded surgical tables or soft mattresses. Without a firm structure beneath the sternum, a significant portion of the compression force may simply move the patient’s body downward rather than compressing the heart between the sternum and thoracic spine.
When feasible, a rigid support, fluid bag, sandbag, gel roll, or positioning device can be placed beneath the sternum to create counter-pressure against posterior thoracic compressions. This stabilization helps convert more compression force into effective cardiac compression and may improve arterial pressure generation during resuscitation.
Step 6: Manage the Airway
Airway management depends largely on the clinical environment.
Many prone arrests occur in intensive care units or operating rooms where the patient already has an advanced airway in place. In these situations, providers should verify tube position and security while continuing ventilations according to current resuscitation guidelines.
If no advanced airway is present, airway access may be difficult in the prone position. Providers should continue chest compressions while simultaneously evaluating whether repositioning is necessary to facilitate airway management.
For additional guidance, see BLS Airway Management Techniques.
Step 7: Apply an AED or Defibrillator
Defibrillation remains a critical component of cardiac arrest management.
When conventional anterior-lateral pad placement is not possible, alternative pad positions may be used. Common approaches include bilateral axillary placement or anterior-posterior configurations designed to direct electrical current through the myocardium.
If the patient can be rapidly and safely repositioned, standard pad placement may be preferred.
For more information, see How to Use an AED During CPR.
Step 8: Continuously Evaluate CPR Effectiveness
High-quality CPR requires ongoing assessment.
In monitored hospital environments, providers should evaluate physiologic indicators that help determine whether prone compressions are generating meaningful circulation. Useful measures include arterial blood pressure waveforms, end-tidal carbon dioxide (EtCO₂), oxygen saturation trends, and signs of return of spontaneous circulation (ROSC).
An increase in arterial pressure or a sudden rise in EtCO₂ may indicate improved perfusion and successful resuscitation efforts.
What Is the Difference Between Prone and Supine CPR?
The primary difference between prone and supine CPR is the direction of compression force.
During conventional CPR, force is applied to the sternum, compressing the heart between the sternum and thoracic spine. During prone CPR, force is applied through the thoracic vertebrae, compressing the heart between the spine and sternum.
Hand placement also differs. Conventional CPR uses the lower half of the sternum, whereas prone CPR typically targets the T8–T9 vertebral region. Airway management, AED pad placement, and overall team logistics may also be more challenging in prone patients.
Despite these differences, the goals remain identical: maintain blood flow to vital organs and maximize the likelihood of return of spontaneous circulation.
Is Prone CPR Effective?
Available evidence suggests that prone CPR can generate meaningful circulation and may be preferable to delaying compressions while repositioning the patient.
Several case reports, physiologic studies, and observational investigations have demonstrated that prone compressions can produce adequate systolic blood pressure, coronary perfusion pressure, and end-tidal carbon dioxide levels. Some studies have even reported arterial pressures equal to or greater than those achieved during conventional CPR.
Successful return of spontaneous circulation and favorable neurologic outcomes have been documented in both surgical and intensive care settings.
Although large randomized controlled trials are lacking, the available evidence supports immediate prone CPR when turning the patient supine would significantly delay treatment.
What Do Current Guidelines Say About Prone CPR?
Major resuscitation organizations recognize prone CPR as a reasonable intervention in selected circumstances.
The American Heart Association (AHA) acknowledges that chest compressions may be performed in the prone position when patients cannot be rapidly turned supine, particularly in operating rooms and critical care environments.
Similarly, the International Liaison Committee on Resuscitation (ILCOR) has reviewed the available evidence and concluded that prone CPR can be considered when immediate repositioning is impractical and compressions can be delivered effectively.
A consistent theme across modern resuscitation guidance is that chest compressions should not be delayed solely for repositioning when immediate prone CPR is possible.
How Can You Tell If Prone CPR Is Working?
One advantage of prone CPR in hospital settings is the availability of advanced monitoring.
Providers should monitor arterial blood pressure waveforms, EtCO₂ measurements, oxygenation data, and signs of return of spontaneous circulation throughout resuscitation.
Persistently low arterial pressures, very low EtCO₂ values, or poor chest wall movement may indicate inadequate compression quality. In such situations, providers should consider repositioning the patient to the supine position if sufficient personnel are available and the benefits outweigh the risks.
Monitoring these physiologic markers helps clinicians make informed decisions about continuing prone CPR versus transitioning to conventional resuscitation.
When Should a Patient Be Turned Supine?
Although prone CPR can be effective, supine CPR remains the standard approach whenever it can be performed safely.
Providers should consider transitioning to the supine position when:
- Adequate personnel are available to safely reposition the patient
- Advanced airway procedures are required
- Defibrillation is difficult to perform
- Compression quality appears inadequate
- Hemodynamic monitoring suggests poor perfusion
- Additional advanced resuscitation interventions are needed
If prone compressions fail to generate adequate arterial pressures or acceptable EtCO₂ values, turning the patient supine should be strongly considered as soon as it can be accomplished safely.
Limitations of Prone CPR
Prone CPR is a valuable resuscitation technique, but it has limitations.
Many providers receive little formal training in prone compressions, making familiarity and confidence potential barriers. Airway access can be difficult, AED placement may require modification, and assessing compression effectiveness may be more challenging than during conventional CPR.
The evidence base for prone CPR is also smaller than that for standard CPR, consisting primarily of physiologic studies, observational data, and case reports rather than large randomized trials.
For these reasons, prone CPR should be viewed as an alternative strategy used when conventional CPR cannot be immediately performed.
Contraindications and Situations Requiring Caution
Prone CPR may not be appropriate in every cardiac arrest scenario.
Providers should exercise caution when compression landmarks cannot be identified, surgical equipment obstructs access to the thoracic spine, or rapid supine repositioning can be achieved without delaying treatment.
Clinical judgment remains essential, and the decision should always prioritize the delivery of effective, uninterrupted chest compressions.
Practical Tips for Healthcare Providers
Successful prone CPR begins long before an actual cardiac arrest occurs.
Hospitals should establish prone arrest protocols, educate staff on thoracic compression landmarks, conduct mock-code simulations, and ensure that teams understand alternative AED pad placement strategies. Facilities that routinely care for prone patients should also develop clear criteria for when repositioning should occur during resuscitation.
Regular training improves team coordination, reduces delays, and helps ensure high-quality CPR regardless of patient positioning.
Healthcare professionals seeking hands-on practice should maintain current BLS Certification Training.
Key Takeaways
Prone CPR is a specialized resuscitation technique used when a patient experiences cardiac arrest while lying face down and immediate repositioning would delay lifesaving treatment. Current evidence and guidance from organizations such as the AHA and ILCOR support initiating chest compressions in the prone position rather than delaying CPR.
Proper hand placement over the T8–T9 vertebral region, adherence to standard compression depth and rate targets, use of anterior counter-pressure when feasible, and continuous physiologic monitoring can help optimize outcomes. While conventional supine CPR remains the preferred standard, every healthcare provider should understand when and how to perform prone CPR safely and effectively.
Frequently Asked Questions
Can CPR be performed on a patient lying face down?
Yes. Prone CPR is an accepted resuscitation technique when turning the patient onto their back would significantly delay chest compressions or create additional clinical risk.
Where do you place your hands during prone CPR?
Hands are typically placed over the mid-thoracic spine at approximately the T8–T9 vertebral level, which usually corresponds to a point just below the inferior angles of the scapulae.
What compression depth should be used during prone CPR?
Current adult BLS targets should be maintained: at least 2 inches (5 cm) but no more than 2.4 inches (6 cm), delivered at a rate of 100–120 compressions per minute.
Is prone CPR recommended by the AHA?
The AHA recognizes prone CPR as a reasonable option when immediate supine positioning is not feasible and delaying chest compressions would be harmful.
Can an AED be used during prone CPR?
Yes. Alternative pad placements, including bilateral axillary or anterior-posterior configurations, may be used when standard anterior-lateral placement is not possible.
Is prone CPR as effective as conventional CPR?
Available evidence suggests prone CPR can generate adequate circulation and favorable hemodynamic parameters. However, conventional supine CPR remains the preferred standard whenever it can be performed without delaying treatment.
How do clinicians know if prone CPR is effective?
Providers may assess effectiveness using arterial blood pressure waveforms, end-tidal carbon dioxide (EtCO₂), chest wall movement, and signs of return of spontaneous circulation.
When should a patient be turned from prone to supine during CPR?
Patients should be transitioned to the supine position when adequate personnel are available, advanced interventions are needed, or monitoring suggests that prone compressions are not generating sufficient perfusion.